Everyone expects pregnancy to be a physiological period and to pass without major problems; both the mother and the baby spend a hopeful and transformative time under the supervision of experts, in good health.
While this is true in most cases, there are serious complications that can turn pregnancy into a high-risk situation. One of these complications is HELLP Syndrome; this is a serious hypertensive disorder in pregnancy that requires rapid diagnosis and treatment.
Why is it Named HELLP?
The name resembles the call for help in English ("help") and in fact, HELLP syndrome is a pregnancy complication that can threaten the lives of both the mother and the baby; therefore, it is considered a true emergency.
However, the name HELLP is actually an English acronym summarizing the three main disorders seen in this disease:
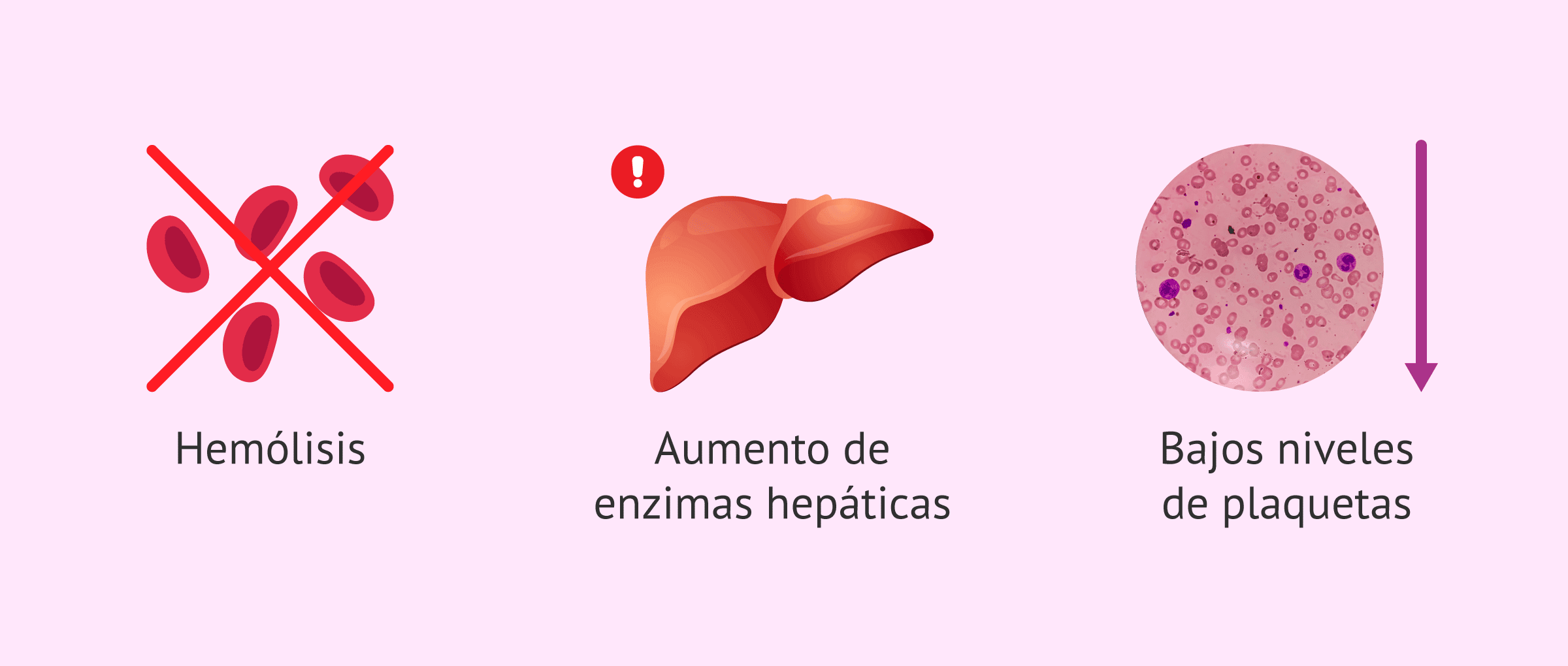
- H – Hemolysis or the breakdown of red blood cells (Hemolysis). This means microangiopathic hemolytic anemia; that is, red blood cells are damaged as they pass through damaged blood vessels.
- EL – Elevated Liver enzymes. This indicates damage to liver cells; these cells may become inflamed and function poorly.
- LP – Low Platelet count. This leads to a condition known as thrombocytopenia; meaning that the number of cells responsible for blood clotting is significantly reduced.
Therefore, HELLP Syndrome is considered a triad characterized by hemolysis, elevated liver enzymes, and thrombocytopenia. Many experts regard this as a severe variant of preeclampsia; however, it may occur with or without significant blood pressure elevation.
What Does This Syndrome Involve?
HELLP Syndrome is a set of symptoms and analytical disorders typically associated with preeclampsia; in most cases, a diagnosis can be made before blood pressure values rise significantly. This can sometimes make immediate recognition difficult.
This is a disease that manifests with various symptoms and until the 1980s, it was not defined as a syndrome with a common basis. The term was introduced by Dr. Louis Weinstein in 1982, who discovered the connection.
Symptoms can vary widely and may sometimes be confused with other common pathologies in pregnancy, such as flu, gastritis, cholecystitis, hepatitis, or even muscle problems. Additionally, in some women, the syndrome may present very mildly or show almost no symptoms at all; this can delay diagnosis.
Among the most common symptoms are:
- Severe discomfort or a general feeling of illness without a clear cause.
- Persistent headache, often resembling that of preeclampsia.
- Nausea, vomiting, or painful indigestion after eating, which can be confused with common digestive disorders.
- Abdominal pain, especially in the upper right part of the abdomen or the stomach area; this occurs due to enlargement of the liver.
- Shoulder pain, sometimes while taking a deep breath, stemming from diaphragm irritation related to the liver.
- Easier bleeding than normal (for example, nosebleeds, bleeding gums, or easy bruising).
- Visual changes, such as blurred vision or seeing "lights" or flashes.
- Swelling in the face, hands, or feet due to fluid retention.
- High blood pressure in most cases, but it may not always be very high initially.
- Severe fatigue and shortness of breath or discomfort while taking deep breaths.
- Rapid weight gain due to excess fluid accumulation during pregnancy.
In addition to the symptoms, abnormalities in the tests are critical for the diagnosis of HELLP syndrome. These include:
- Elevated liver enzymes (transaminases, LDH, etc.), indicating liver damage or inflammation.
- Destruction of red blood cells (hemolysis), evaluated with parameters such as bilirubin, LDH, haptoglobin, and peripheral blood smear.
- Decrease in platelet count; the severity of the syndrome is classified according to the degree of decrease. The most severe case is when platelets fall below 50,000.
- Significant protein loss in urine (proteinuria), often associated with preeclampsia.
- Coagulation disorders, associated with the risk of bleeding or disseminated intravascular coagulation.
In some cases, conditions where the complete triad is not met (for example, low platelet count and high liver enzymes present, but no hemolysis shown) are referred to as incomplete HELLP syndrome. Still, these incomplete forms require the same level of monitoring and attention as complete forms.
Is It Common?
Fortunately, no. The occurrence of HELLP syndrome is rare: it is seen in approximately 1 to 2 in every 1,000 pregnancies in the general population.
However, if we focus on women with preeclampsia, the risk significantly increases: 10 to 20% of women with preeclampsia are at risk of developing HELLP syndrome. Therefore, monitoring blood pressure and urine throughout pregnancy is very important.
Despite its low prevalence, HELLP syndrome is considered a serious complication that carries the risk of maternal and perinatal mortality if not diagnosed and treated in time. The main causes of complications in the baby are premature separation of the placenta, placental insufficiency, and extreme prematurity.
In most cases, when delivery occurs and the complications are properly managed, the syndrome tends to resolve in the days following delivery; however, recovery may require several days of observation and analytical checks.
When Does It Occur?
It usually occurs from the 26th week of pregnancy, most commonly in the third trimester, but can also be seen in a few cases in the second trimester.
Additionally, it can occur after delivery (postpartum HELLP syndrome); this is less common but very important to recognize. In these cases, the woman may feel quite well during labor, but may begin to deteriorate in the following hours or days and may experience abdominal pain, discomfort, nausea, increased blood pressure, or analytical abnormalities.
Women who have experienced preeclampsia or HELLP syndrome require special monitoring during pregnancy and the postpartum period; because the risk of experiencing late complications is higher.
If a mother experiences this syndrome, she is more likely to experience it again in subsequent pregnancies. The risk of recurrence is estimated to be between 20 and 30%; if the syndrome occurred early (in the second trimester or before the seventh month), the likelihood of recurrence can rise to 60%. Therefore, closer prenatal monitoring and observation in high-risk units are recommended for subsequent pregnancies.
Risk Factors for HELLP Syndrome
Not all women have the same risk of developing this complication. Although it can be seen in women without a history, several factors that increase the likelihood have been identified:
- Having had HELLP syndrome in a previous pregnancy is one of the most important risk factors.
- Experiencing preeclampsia or eclampsia in the current pregnancy.
- Family members with a history of HELLP syndrome or preeclampsia (affected mother or sisters).
- Chronic hypertension or previous blood pressure disorders.
- Multiple pregnancy (twins, triplets, etc.).
- First pregnancy, especially in women with other risk factors.
- Advanced age or very young motherhood, especially in pregnancies during adolescence or from age 35 onwards.
- Autoimmune diseases, such as antiphospholipid syndrome or other coagulation disorders.
Although these factors increase the risk, the absence of these factors does not mean that the syndrome will not occur; therefore, the importance of routine checks in all pregnancies is significant.
Is It Preventable?
Definite prevention is quite difficult, because the exact causes triggering HELLP syndrome are not fully known. This is related to a disorder in the placenta and the mother's blood vessels; it is associated with endothelial damage and micro-thrombus formation, but the exact mechanism is still being researched.
Still, there are some measures and control precautions that can help reduce the risk or especially to make an early diagnosis of the problem to prevent serious complications:
- Being in good physical shape before and during pregnancy and having an appropriate weight, following expert recommendations.
- Having all medical checks during pregnancy on the specified dates, with both the gynecologist and the midwife.
- Regularly attending check-ups, where blood pressure measurements are taken and fetal well-being is monitored.
- No blood or urine tests should be done without the specialist's recommendation, as most of the time the first symptoms appear analytically.
- Previous history of HELLP syndrome, preeclampsia, or other hypertensive disorders in previous pregnancies or in the family should always be reported.
- Knowing emergency signals (severe abdominal pain, severe headache, blurred vision, severe nausea, bleeding, etc.) and consulting the emergency service when they occur.
Currently, there is no strategy to completely prevent this pathology; however, being well-informed, maintaining checks, and acting quickly against symptoms can make a difference in detecting the syndrome at early stages and receiving appropriate treatment in a timely manner.
Does Blood Pressure Always Rise?
There is almost always some degree of blood pressure elevation, but in some women, it may occur after other disorders arise or may be relatively mild at first.
In many cases, the diagnosis is primarily made due to analytical disorders, rather than blood pressure values. Therefore, it is very important never to skip the recommended blood and urine analyses during pregnancy or the postpartum period.
Additionally, HELLP syndrome can be confused with other diseases such as lupus, immune thrombocytopenic purpura, acute hepatitis, viral infections, or gallbladder problems. A comprehensive evaluation by the medical team (history, physical examination, and additional tests) is key to distinguishing it from other conditions associated with abdominal pain, fever, or platelet disorders.
Is There a Treatment?
Treatment depends on the symptoms, the severity of the condition, and the gestational week at which the diagnosis is made. It should always be carried out in a hospital setting, with a multidisciplinary team (gynecologists, anesthetists, intensive care specialists, neonatologists, hematologists).
The disease does not resolve before the end of the pregnancy. Therefore, in most cases, the definitive treatment is the termination of the pregnancy. If symptoms worsen and pose a danger to the mother or baby, inducing labor or performing a cesarean section may often be necessary.
While evaluating and preparing for the termination of the pregnancy, other supportive treatments and checks are performed:
- Hospitalization for close monitoring of the mother and baby.
- Medications to control high blood pressure.
- Medications to prevent seizures if there is a risk of eclampsia (for example, magnesium sulfate).
- Corticosteroids to support the maturation of the baby's lungs if preterm birth is anticipated.
- Platelet or blood transfusion if there is a very low platelet count or significant anemia.
- Monitoring of fluid balance and lung function to prevent pulmonary edema.
- Admission to the intensive care unit if the condition worsens or if there are serious complications (such as disseminated intravascular coagulation, kidney or liver failure, etc.).
- Monitoring of kidney, liver, and coagulation function through serial analyses.
- Close monitoring in the postpartum period, as the syndrome may temporarily worsen after delivery.
In some cases, if the pregnancy is very early and the mother is stable, the team may consider delaying the termination of the pregnancy for a few days; this is done to improve the respiratory prognosis of the fetus by administering corticosteroids, always under very strict monitoring. However, if the life of the mother or the baby is at risk, the priority is to expedite delivery.
How Will My Delivery Be?
In mild cases, if there is no emergency and obstetric conditions are suitable, there may be an option for induction of vaginal delivery. In these cases, the use of epidural analgesia is recommended (if platelet count permits), and the mother's vital signs and fetal well-being must be monitored very closely.
On the other hand, if any signs of emergency arise (analytical deterioration, severe pain, bleeding, fetal distress, etc.), an emergency cesarean section will likely be recommended. In this case, specialists will carefully assess the safest type of anesthesia based on platelet levels and bleeding risk; in some cases, general anesthesia may be necessary. Additionally, specialists will evaluate the most appropriate surgical strategy and type of incision based on platelet count and bleeding risk; if necessary, a platelet transfusion may be performed prior to the intervention.
The location where the delivery will take place is also important: the delivery should occur in a hospital with intensive care units, as the mother and baby may require special support in the postpartum days.
Most babies born in the context of HELLP syndrome have a good prognosis when advanced neonatal care is provided. Their development primarily depends on the gestational week at birth and birth weight; the maturity of their lungs and other organs is also important.
Knowing HELLP syndrome, its most characteristic symptoms, risk factors, and the importance of medical check-ups throughout pregnancy enables many mothers to respond promptly to emergency signals and seek advice without delay. Although it is a rare complication, its potential seriousness shows that information, prevention, and close monitoring are essential to maintaining the health of both mother and baby with the support of the healthcare team.






































Comments
(8 Comments)